 Written By: Dr. Suseela Kiyyath (MBBS, MS)
Written By: Dr. Suseela Kiyyath (MBBS, MS)
What Are Uterine Fibroids?
Fibroids are non-cancerous growths that develop in the muscle layer of the uterus. Fibroids can rarely detach and can be seen attached to the connective tissue( broad ligament) near the uterus. Fibroids are also known as leiomyoma or simply myoma. The growth consists of muscle and fibrous tissue. Their size can vary from a few millimeters to 15-20 centimeters.
Uterine fibroids are the most common non-cancerous growth in the females of the reproductive age group.
Causes Of Uterine Fibroids:
The exact cause of fibroids is unknown, but they have been linked to estrogen. Oestrogen is the female reproductive hormone produced by the ovaries. Fibroids usually develop during women’s reproductive years (16-50) when estrogen levels are highest. They most often occur in women aged between 30-and 50 years. This is because fibroids are so common, with around 1 in 3 women developing them at some point in their life. They tend to shrink after menopause( the permanent cessation of monthly menstruation) when low estrogen levels.
Fibroids are more frequent in women of African-Caribbean origin.
It is also more common in overweight or obese women( being fat increases the level of estrogen in the body).
Women who have had children have a lower risk of developing fibroids, and the risk further declines with the number of children they have.
Studies have found that fibroids respond abnormally to
progesterone( another female reproductive hormone).
Long-term use of oral or injectable contraceptives may lower the risk of fibroids.
Fibroids are more common if another family member has a similar history.
Use of soybean milk and vitamin D deficiency is also associated with increased occurrence of fibroid uterus.
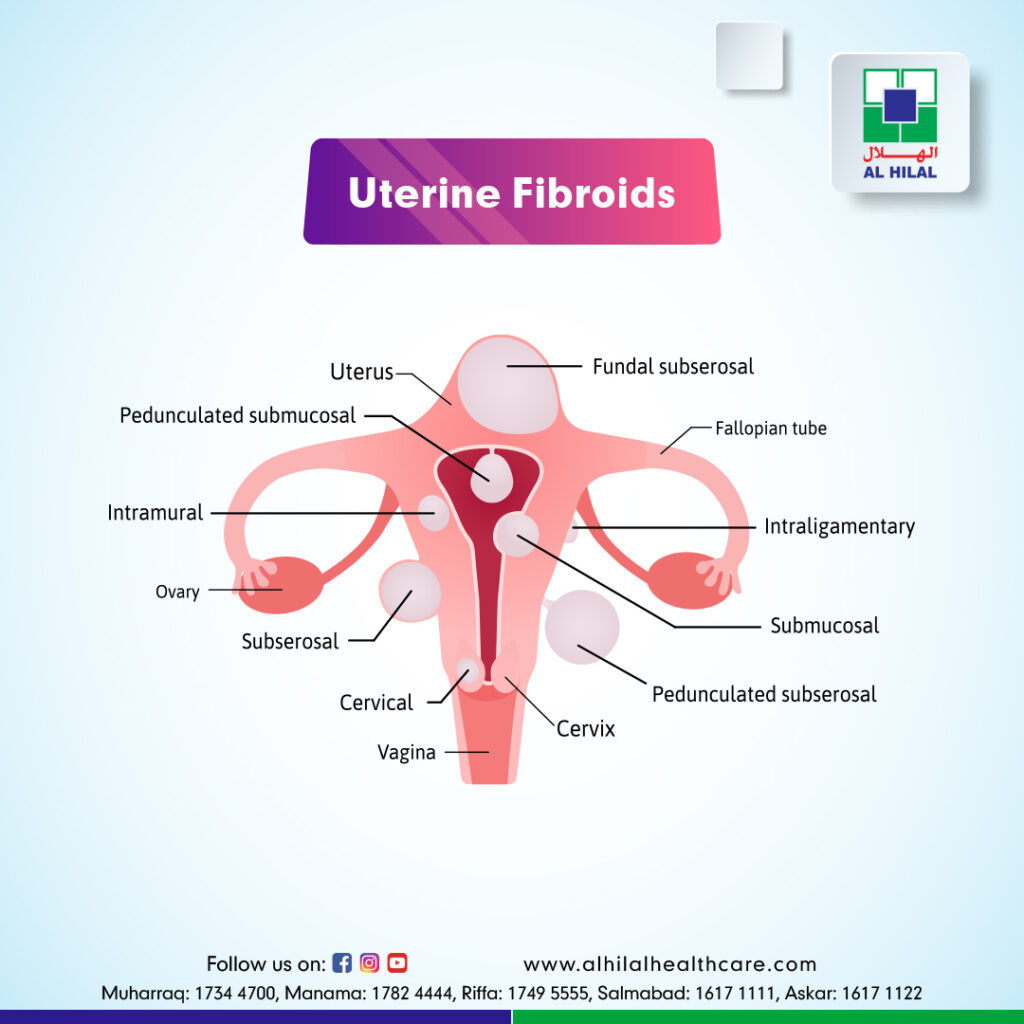
Types Of Uterine Fibroids:
The main types of fibroids are :
- Intramural fibroids are the most common fibroids that remain confined to the uterine contour without expanding locally into the uterine cavity or towards the space outside the uterus.
- Subserosal fibroids expand towards the abdominal cavity around the uterus and can become very large. Sometimes they are attached with only a narrow stalk of tissue to the womb, then described as pedunculated fibroids.
- Submucosal fibroids are the fibroids that grow towards the uterine cavity.
Symptoms Of Uterine Fibroids:
2/3rd of women do not have any symptoms. They are then diagnosed by chance during a routine gynecological check-up or ultrasound abdomen done for some unrelated complaint. The most common symptom is heavy menstrual bleeding. Others may experience painful periods, non-cyclical tummy pain, low backache, urinary frequency, urinary retention, recurrent urinary tract infection, constipation, discomfort during sex, chronic vaginal discharge, intermenstrual bleeding, and fullness of lower abdomen, or distended abdomen. Fibroids can cause abortions, infertility, and premature labor in rare cases.
Uterine Fibroids And Pregnancy:
Submucous fibroids(located very close to the uterine cavity) can block the fallopian tube. Fallopian tubes are narrow tube-like extensions from either side of the upper part of the uterus towards the right and left ovaries through which sperms and ovum travel to meet each other for fertilization( union of sperm and ovum). Fertilized ovum travels through the fallopian tube to get implanted( attached) to the uterine lining. Fibroids can also prevent the sperm from reaching the egg. Thus fibroids can result in infertility ( inability to get pregnant). Complications occur in about 10-40% of cases with fibroid complicating pregnancy. Ectopic pregnancy ( implantation of a fertilized egg outside the uterine cavity) is more common in women with fibroids. Sub mucus fibroids can also result in recurrent abortions( 2 fold in symptomatic fibroids) and premature labor. Sometimes fibroids can lead to problems with the baby’s development or difficulties during work. Large fibroids may prevent expected vaginal delivery, and a cesarean may be necessary. In addition, Fibroids can contribute to excessive postpartum bleeding.
Fibroids can undergo degeneration during pregnancy, resulting in abdominal pain and fever.
Fibroids may increase in size during pregnancy.
Diagnosis Of Fibroids:
As the majority of women are asymptomatic, they may not get diagnosed.
The diagnosis is usually made through pelvic examination and ultrasound examination of the abdomen in suspected patients. However, many asymptomatic cases are diagnosed accidentally during the ultrasound abdomen for other suspected conditions. Sometimes they get incidentally detected during other abdominal surgeries also. MRI, CT, Hysteroscopy( a thin, flexible tube with a light source and camera introduced through the vagina into the uterine cavity), Hysterosalpingography( known as HSG and usually done as a part of the evaluation of infertility in which a contrast material is injected first and X rays of the uterus are taken), Sonohysterography( here saline is injected via a catheter into the uterine cavity which will help to obtain a clearer image of the uterine cavity in the subsequent ultrasound scanning) and laparoscopy are the other modalities through which uterine fibroids may be diagnosed. The definitive confirmation of the fibroid uterus is made by microscopic examination of a tissue sample obtained through hysteroscopy or laparoscopy, myomectomy, or hysterectomy specimen.
Who Needs Treatment For Uterine Fibroids?
Fibroids don’t need to be treated if they are not causing symptoms. Asymptomatic fibroids can be followed up by pelvic examination and ultrasound at regular intervals to rule out any sudden increase in size. This may point toward leiomyosarcoma(uncontrolled malignant growth of smooth muscles), which can be mistakenly diagnosed as uterine fibroid initially. Treatment of fibroids is planned based on the symptoms and varies according to the size, number, and location of fibroids and the desire for pregnancy and uterine preservation.
Treatment may be warranted in cases with moderate to severe dysmenorrhea( pain during menstruation), mild to severe abdominal pain, menorrhagia, infertility( where other causes have been ruled out) , recurrent abortions, pressure symptoms like heaviness abdomen, urinary retention with or without recurrent urinary tract infection(urinary retention creates urinary stasis which in turn help the bacteriae to multiply and cause illness), hydronephrosis( hydronephrosis is the swelling of kidneys which the pressing of ureters can cause by fibroids located at specific locations by lateral extension and this can affect kidney function later).
Treatment Of Uterine Fibroids:
Levonorgestrel intrauterine system (LNG-IUS-a plastic T-shaped device placed in your womb that slowly releases the progesterone hormone levonorgestrel)makes the uterine lining thinner and bleeding becomes lighter. This provides contraception( prevention of pregnancy) also. The side effects include irregular bleeding that may last for more than six months, acne, headache, breast tenderness, and in some cases, absent menses.
If LNG-IUS is not suitable( for example, if contraception is not desired or cannot be inserted due to distorted uterine cavity due to fibroid itself)or for immediate treatment, tranexamic acid injection or tablets may be considered 3 or 4 times a day for up to 4 days for heavy bleeding.
Non-steroidal anti-inflammatory drugs( NSAIDs) such as mefenamic acid and ibuprofen can be taken three times a day for a few days. They work by reducing the production of prostaglandins (a locally produced hormone-like substance) linked to heavy bleeding and pain. However, they do not provide contraception. Indigestion and diarrhea are common side effects and sometimes result in an allergic reaction.
The contraceptive pills can also help in reducing the bleeding and pain associated with fibroids.
An oral progestogen ( a synthetic progesterone female sex hormone) taken from days 5 to 26 of your menstrual cycle(counting the first day of your periodic bleeding as day 1) can help reduce the bleeding by making the uterine lining thinner. This, in addition, reduces the chances of conceiving, but this is not a form of contraceptive method advised. The side effects of oral progesterone include weight gain, breast tenderness, and short-term acne.
Injected progesterone(DMPA) acts similar to LNG- IUCD. This provides contraception too.
GnRH analogs such as goserelin acetate work by affecting the pituitary gland ( a pea-sized gland located at the bottom of the brain which controls the hormone production from the thyroid, ovaries, testes, and adrenals), which in turn stops the ovaries from producing estrogen resulting in shrinkage of fibroids. The menstruation stops temporarily. They are not used as contraceptives. They are given as injections. They reduce the pressure symptoms like urinary frequency and constipation caused by fibroids. They are generally used on a short-term basis to delay the surgery until the patient is fit for the surgical procedure. This can provide time to build up hemoglobin lost during heavy periods naturally. But these drugs can cause menopausal symptoms like hot flushes, increased sweating, muscle stiffness, and vaginal dryness. It can also result in osteoporosis( bone loss). They can be combined with HRT( hormone replacement therapy) to prevent these side effects.GnRH agonists, if used alone, are prescribed only on a short-term basis( a maximum of 6 months at a time). The fibroids may grow back to their original size after the cessation of this therapy.
Ulipristal acetate( Esmya) is selective progesterone ( female hormone) receptor modulator prescribed only to treat fibroids with moderate or severe symptoms in premenopausal women for surgical procedures, including uterine artery embolization, are not appropriate or have not worked. This is because there is a risk of severe liver damage and liver failure. The symptoms of liver failure include tummy pain, nausea, vomiting, loss of appetite, tiredness, yellowing of the white part of the eye, and dark pee. These can appear even after stopping ulipristal acetate. Therefore, the drug is given in intermittent courses—each with a daily 5 mg dose for three months per course.
Surgical procedures may be needed for severe symptoms if the medical methods fail. These include hysterectomy and myomectomy. Hysterectomy is the surgical procedure to remove the womb. This is the most effective method to prevent fibroids from coming back. This procedure may be recommended if you have large fibroids or severe bleeding and do not wish to have more children. This can be done under spinal, epidural, or general anesthesia. The smaller-sized uterus can be removed vaginally or through a laparoscopy-assisted vaginal procedure. Uteri of any size can be removed through a laparotomy( a surgery in which the abdomen is opened through a large incision on the anterior aspect of the abdominal wall).
Myomectomy is a surgery in which only the fibroid is removed, and the rest of the uterus is left-back. This is preferred if one needs to preserve the uterus. But this is not suitable for some cases depending on the number, size, and location of the myomas. This is carried out under general anesthesia and can be done as keyhole surgery or open surgery. Submucosal fibroids can also be removed hysteroscopically. Hysteroscope is a thin telescope passed inside the uterus through the vagina, and no incisions are required on the abdomen. Again, this procedure can be done under general anesthesia (mainly) or local anesthesia. There can be mild bleeding per vagina after the process for a few weeks, which should stop within a few weeks. Hysteroscopicmorcellation is another method in which a morcellator is used to remove the myoma, and the risk of injury to the womb is lesser. But as this is a new technique, evidence of its overall safety and long–term effectiveness is limited.
Novel methods to treat fibroids include Uterine Artery Embolization( UAE), MRI-guided percutaneous laser ablation, MRI-guided transcutaneous focused ultrasound, and radiofrequency ablation( RAF).
UAE is an alternative procedure to hysterectomy or myomectomy. It may be recommended for women with large fibroids. The blood vessel(uterine artery) to the fibroid is blocked through a catheter guided through a blood vessel in the leg under local anesthesia under X-ray guidance. It is possible to have a pregnancy after this procedure, but the overall effect of the process on fertility and pregnancy is uncertain. In addition, the long-term benefits and risks of MRI-guided treatment methods are unknown, and those methods are not yet widely available. RFA can be performed laparoscopically, transvaginally, or transcervical.
Iron supplements, oral or intravenous, are an integral part of supportive management to deal with blood loss and resulting anemia.
Intravenous fluids and blood transfusion may be required in severe cases.
Results Of Treatment For Uterine Fibroids:
LNG- IUCD reduces fibroid-related menorrhagia more efficiently than combined oral contraceptive pills(90.9% vs13. 4%). So many times, surgery can be avoided with LNG-IUCD, and the same can be offered before surgery to reduce bleeding. Changes in uterine size are inconsistent with LNG-IUCD.
There is a lack of high-quality evidence supporting oral or injectable progestogens in bleeding related to fibroids, which may be associated with microscopic changes that may mimic malignancy.
Non-steroidal anti-inflammatory drugs ( ibuprofen, mefenamic acid) may result in a 36%reduction in fibroid associated bleeding)
Tranexamic acid reduces blood loss in 40% to 50%of women and may cause damage to fibroids, significantly larger ones.
GnRH agonists are primarily used preoperatively, and they reduce uterine bleeding in 89%cases and fibroid volume by 50-72%cases. The median time to control bleeding is 21 days with leuprolide acetate( a GNRH agonist). Although highly effective, side effects limit its use.
Ulipristal acetate(UPA) is found to control uterine bleeding in 90-98%cases, and the median time to control bleeding is 5-7 days, but the severe side effects limit its use. However, pregnancies after UPA treatment have been reported.
Approximately 50%of women with fibroid and infertility conceive after myomectomy(fibroid removal).
Uterine Fibroids Treatment In Bahrain:
Al Hilal Hospital is the largest and fastest-growing chain of private healthcare providers in Bahrain, with five branches. Al Hilal Healthcare Group is committed to providing high-quality healthcare services at an affordable price to the people of Bahrain through a combination of superior medical technology and excellent clinical services. Its vision is to be the largest healthcare service provider in the region by catering to the needy at the most affordable rates.
The Department of Obstetrics and Gynecology has been providing comprehensive healthcare for women. As a result, the healthcare group has successfully treated many Uterine Fibroids patients and provided them with a complete cure for the fibroids.
Uterine Fibroids Specialist In Bahrain:
Al Hilal Healthcare group is equipped with several well-qualified and experienced Gynecologists who are specialists in treating Uterine Fibroids
